Dosimetric unknowns in patient setup
Treatment planning is performed on a static CT dataset, capturing a single snapshot. Surface Guided Radiation Therapy (SGRT) technologies have become instrumental in helping position patients consistently, using surface metrics to guide alignment. Yet, typical SGRT tolerances – often set generically at 3–5 mm and 3 degrees – are rarely customized to individual patients and their unique anatomical presentation. These thresholds don't reflect the actual dosimetric consequences of deviations for a given patient.
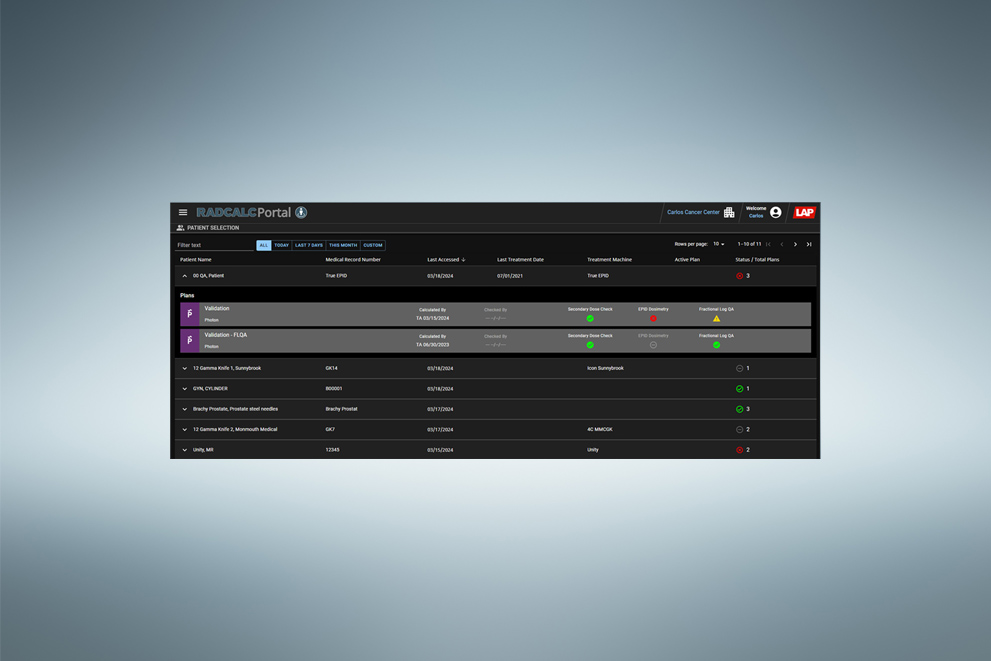
Paired with RadCalc’s 3D QA suite, we’re creating an integrated workflow to expose potential errors, before delivery.
The challenge is recognized – but not universally solved
Unseen dosimetric uncertainty is now widely recognized across the field. Modern radiotherapy systems increasingly incorporate online adaptive workflows that account for daily anatomical variations by aligning the day’s image to a reference and adjusting the treatment plan accordingly. However, these solutions require significant infrastructure. Many clinics lack such technology, yet still face the same challenges of anatomy-driven dose variability.

What our customers say
- “The real game-changer is how your solution bridges SGRT with RadCalc’s dose calculation algorithms—that’s the icing on the cake.”
- “I think the value is that you provide a more individual tolerance… It simplifies the workflow.”
- "What you guys are doing {in displaying 3D projected dose} is evaluating it upfront instead of after the fact."
Making precision effortless

More about dose-aware Surface Guided Radiation Therapy
What is the new more in SGRT?
LAP is developing a next-generation dose evaluation module within RadCalc that uses SGRT surface data to provide clinicians with dosimetric insights that consider the daily variation in patient positioning. It will empowers clinicians with the opportunity to uncover undesirable dose deliveries before they deliver them.
How does the new more in SGRT add value to my clinical workflow?
Conventional setup verification (e.g., SGRT or CBCT alone) confirms surface and anatomical alignment but offers no insight into the dose being delivered to today’s patient setup. The new more in SGRT addresses this critical blind spot by showing how variations in patient setup, weight, or anatomy affect dose delivery — before and after treatment.
What treatment machines will the new more in SGRT work with
RadCalc’s new module will support workflows for pretreatment dose evaluation for all standard C-arm linac configurations.
How fast are the dose recalculations with RadCalc’s fMC?
The new more in SGRT will recalculate your clinical plans using RadCalc’s new fast Monte Carlo dose engine in typically 30 seconds. Find out more here.
Is it customizable to our clinical protocols?
Yes, you can define: unique clinical protocols, what structures are monitored, which metrics are flagged and thresholds for pass/warning/failures
Are there special hardware requirements for the new more in SGRT?
Yes. Dedicated calculation hardware will be required for the fast Monte Carlo dose calculations.
Will therapists be making dosimetric decisions on their own?
No. As part of LAP’s initial setup for RadCalc’s newest module, physicists will be determining guiderails for the treatment team. These guiderails are intended to lay a foundation for what is acceptable during the daily treatment sessions. If conditions develop which are outside of the acceptable guiderails, physicists will have the ability to remotely access the same information the therapists are seeing at the treatment console to assist with decision making.
What does our clinical team do in the event of an undesirable dose evaluation?
RadCalc’s new TrueDose module will include a full record of the previously treated fractions for physics to review during the decision-making process
German Patent Application No. 10 2023 115 102.9, PCT Patent Application No. EP2024/065566, US Patent Application No.19/144,366
The information provided contains forward-looking concepts and is intended for illustrative purposes only. All referenced design elements, functionalities, and specifications are preliminary and subject to change without notice.